- Call or text today
- 1-508-8822542

Short Dental Implants: What Are They and When Are They Preferred?
Short Dental Implants: What Are They and When Are They Preferred?
Dental implants come in two options: long (traditional) ones or short ones. However, when is one preferred over the other, and who might benefit from a short dental implant?
In many cases, short dental implants offer a solution for when traditional implants are impossible to place, such as when there is not enough bone. Their smaller size also allows them to avoid nearby nerves without a need for complex surgery. However, they are not the best option in every situation, so to choose the best implant type for you, your doctor will take into consideration your unique scenario and oral structures.
Continue reading to learn more about short dental implants and what cases might make you a good candidate for them.
What are Short Dental Implants?
Generally, a short dental implant is ≤ 8 mm long, and anything ≤ 6 mm long is considered extra short. In comparison, traditional implants range from 8 mm to 15 mm, as this resembles the natural length of the tooth’s root. However, putting in a dental implant this long is not always best.
3 Cases Where Short Dental Implants Are Preferred
Whether or not you would benefit from a short dental implant requires your dentist to consider your unique case and whether your circumstances would see better success with a short implant. The following are three scenarios that, if applicable, may make you a good candidate for a short dental implant.
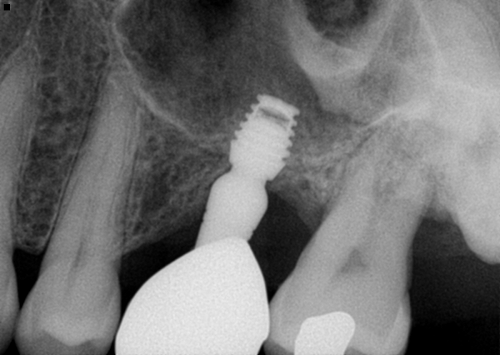
When the Upper Jawbone Is Limited Because Of Low Sinus Floor
Sinus lifting is a surgical procedure in which the bone tissue of the upper jaw is increased to a higher thickness. The purpose of sinus lifting is to provide more bone for the traditional dental implant—often 10 mm long—to anchor on to. If sinus lifting cannot be completed when the upper jawbone is of a short height, it is impossible to place an traditional implant. In these cases, short dental implants are a perfect solution. (Figure 1)
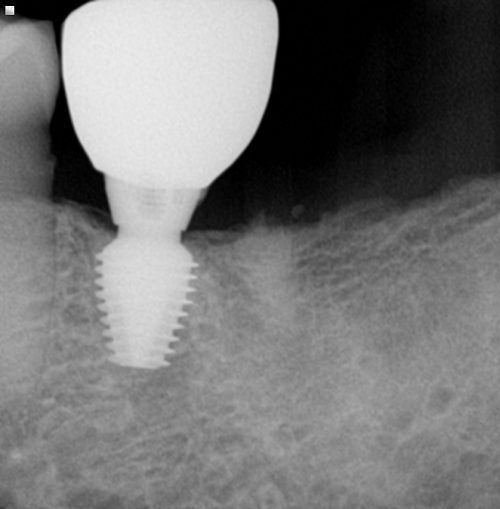
Major Defects in the Low Alveolar Crest
The alveolar crest is the topmost part of the alveolar process, or the extension of the mandible and maxilla that holds the tooth in place. For those with periodontal disease, the alveolar crest is often the first part of the alveolar process that is damaged. Consequently, the alveolar crest is also the first bone that is lost.
When there is a bone deficiency in the alveolar crest, short dental implants offer an alternative to complex surgeries, such as vertical augmentation. These surgeries have a high risk of complications, such as nerve damage and a loss of jaw sensitivity, and even in the cases of no complications, patients can expect a long period of severe pain and discomfort. In comparison, short dental implants avoid the need for these complex surgical operations. ( Figure 2)
Those Who Do Not Want Bone Augmentation Surgery
There may be many reasons why someone does not want to undergo bone augmentation surgery, such as age, the presence of chronic diseases such as diabetes, financial reasons, a fear of complications, or a lack of time. For reference, vertical augmentation can take a year or more from the first surgery to when the implant is placed.
With there also being a risk of complications with these surgeries, short dental implants offer an alternative that doesn’t take as long, has minimal risk of complications, and has a survival rate of more than 90%.
In our office, we find that most senior patients who are edentulous prefer short implants—they are a great solution that restores the whole mouth with much fewer surgical procedures.
Advantages of Short Dental Implants
The success rates of short dental implants are very favorable. One study in the Journal of Oral and Maxillofacial Surgery found that, after one year, only 59 out of 2,573 short implants failed. Yet another study spanning 10 years saw a survival rate of 98.3%.
Additionally, short implants have a slightly higher success rate when utilized in the lower jaw compared to the upper jaw. Since they are placed in the lower jaw more often, as nearby nerves are more common in the lower jaw, these higher success rates are advantageous.
Yet another advantage of short dental implants is that they can be utilized in complex situations when a long implant is not possible. This can include situations where there is minimal bone or where it is difficult to reach. Furthermore, short dental implants make it so that, even if there is limited bone around the molar and premolar teeth, a surgical procedure of bone graft does not always need to be completed.
Disadvantages Of Short Dental Implants
The greatest disadvantage of the short dental implant is found within its name: it’s shorter than a traditional implant. Unfortunately, while this allows it to avoid hitting a nerve, this also means that the short dental implant has less room for anchorage. Because of this, they are not ideal for supporting individual crowns, especially where the teeth experience more bite pressure. Instead, short dental implants work best where prosthetic teeth are connected, as it offers them more strength.
Are You a Good Candidate for Short Dental Implants?
Short dental implants show their strengths in many situations. They offer an implant option that is appealing when there is concern about a nearby nerve, as they can be implanted without the patient needing to undergo nerve repositioning surgery. They also show advantages in hard-to-reach locations or when there is insufficient bone and a bone graft is not an option.
However, short dental implants are not ideal for places with high bite pressure or single crowns because they don’t have as much anchorage.
Considering this, there are specific scenarios where a short dental implant can be ideal. Inquire with us about a free implant consultation to see if you’re a good candidate for short dental implants.
References
Bataineh, A. B., & Al-dakes, A. M. (2016). The influence of length of implant on primary stability: An in vitro study using resonance frequency analysis. Journal of Clinical and Experimental Dentistry. https://doi.org/10.4317/jced.53302
Atieh, M. A., Zadeh, H., Stanford, C. M., & Cooper, L. F. (2012). Survival of short dental implants for treatment of posterior partial edentulism: a systematic review. The International journal of oral & maxillofacial implants, 27(6), 1323–1331.
Lai, H. C., Si, M. S., Zhuang, L. F., Shen, H., Liu, Y. L., & Wismeijer, D. (2013). Long-term outcomes of short dental implants supporting single crowns in posterior region: a clinical retrospective study of 5-10 years. Clinical oral implants research, 24(2), 230–237.